INTRODUCTION
Cervical radiculopathy typically presents with neck pain, arm pain, paresthesia, numbness, or motor weakness due to inflammation or compression of the cervical nerve root [1,2]. The most common causes of cervical radiculopathy are cervical disc herniation and cervical spondylosis [3,4]. While anterior cervical discectomy and fusion (ACDF) has been considered the gold standard in managing cervical radiculopathy [5], the literature shows a variety of complications associated with the procedure, including adjacent segmental diseases, pseudoarthrosis, postoperative dysphagia, vascular injury, recurrent laryngeal nerve palsy, cerebrospinal fluid leakage, and hematoma [6-8].
Traditional posterior cervical foraminotomy (PCF) was developed long before ACDF and is recognized as a simple and effective surgical treatment for cervical radiculopathy [9]. It avoids the complication associated with anterior approach and preserves the mobility of the operated segment [9-11]. However, traditional PCF requires a large surgical incision and massive dissection of the posterior neck musculo-ligamentous structures. The extensive soft tissue damage resulting from this approach may lead to severe wound pain, delayed recovery, and a high incidence of postoperative neck pain [9,12,13]. In addition, excessive facet joint destruction may lead to the concerns for post-decompression segmental instability which requires a second operation for reconstruction [14,15].
In recent years, spine surgeons have paid attention to the biportal endoscopic technique. This technique is performed through two independent portals with continuous irrigation of normal saline, providing hydrostatic pressure to suppress bleeding and carry away bone debris and oozing. Combined with a high-resolution endoscope, the biportal endoscopic technique provides a clear, bright, and magnified surgical field of view, enabling surgeons to perform delicate surgical procedures without excessive soft tissue damage. This minimally invasive technique has been applied to address a variety of spinal pathologies, such as discectomy for lumbar disc herniation, laminotomy for degenerative lumbar spinal stenosis, and lumbar interbody fusion for disc degeneration or spondylolisthesis, all of which have demonstrated good clinical efficacy [16-21].
Recently, we have performed biportal endoscopic posterior cervical foraminotomy (BEPCF) in patients with unilateral cervical radiculopathy, attempting to make traditional PCF a minimally invasive procedure. The purposes of the study are to describe the surgical techniques in detail, and to evaluate the preliminary clinical outcomes.
MATERIALS AND METHODS
1. Patient Selection
This case series included 36 consecutive patients who received 38 segments of biportal endoscopic posterior cervical foraminotomy (BEPCF) between November 2020 and June 2022. The patients were 24 males and 12 females with an average age of 56.8 years (range 39–63 years).
Indications for BEPCF were radicular arm pain, single or multiple cervical radiculopathies due to foraminal stenosis, with persistent symptoms for more than three months and failure of conservative treatment. We excluded patients with segmental instability, kyphotic sagittal alignment, and prior surgeries in their cervical spines. Patients with central canal stenosis and myelopathy, characterized by abnormally increased deep tendon reflexes, hyperclonus of ankles, abnormal Babinski reflexes, or gait disturbance were also excluded. Thirty-four patients received one-segment decompression, while two patients received two-segment decompression (Table 1). All surgeries were performed by the senior author in a single medical center.
2. Evaluation of Clinical Data and Outcomes
We obtained demographic and clinical data, as well as treatment outcomes, through chart reviews. All patients underwent baseline evaluation before surgery, followed by evaluations at 1 month, 3 months, 6 months, and 1 year after surgery, and then annually thereafter. Outcome measures included the visual analog scale (VAS) for arm pain, the neck disability index (NDI) for disability [22], and the modified MacNab criteria for the overall outcomes [23].
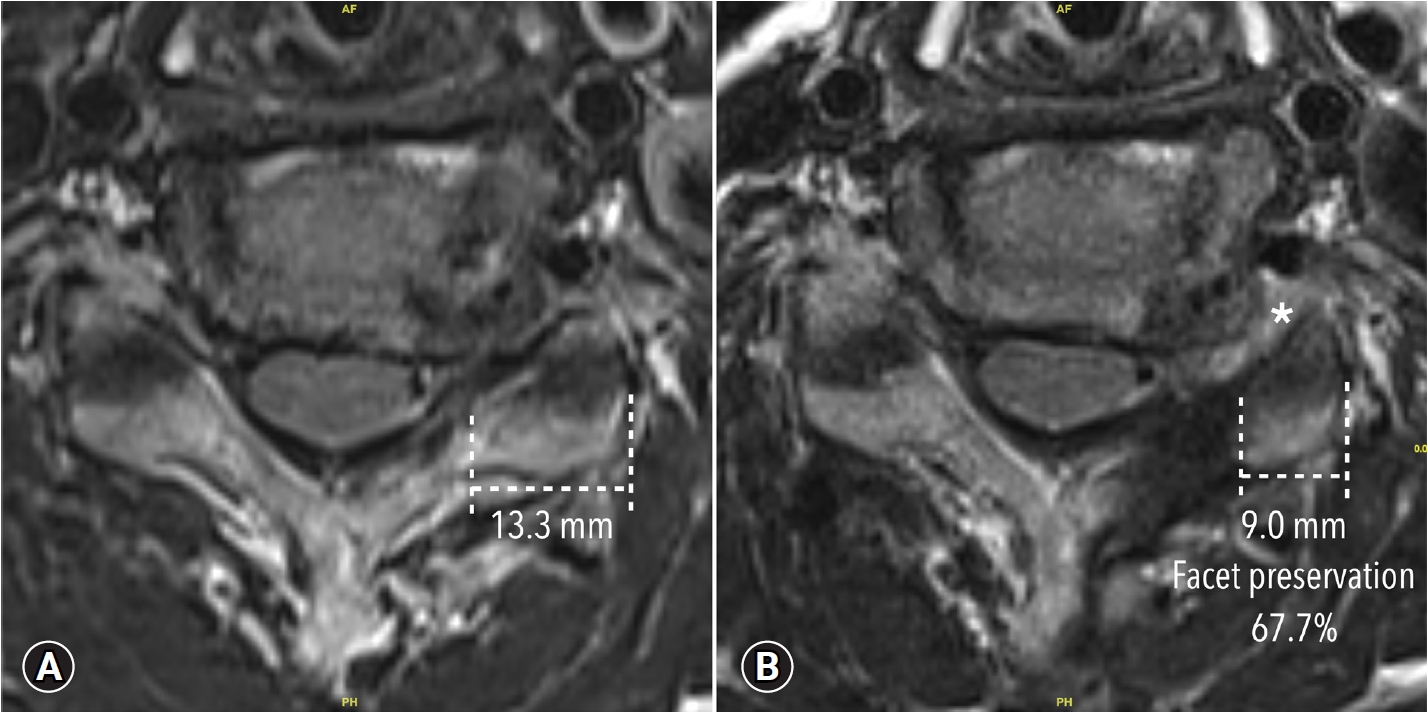
All patients underwent plain X-rays of AP, lateral, oblique, and dynamic lateral views before the surgery, as well as at 3 months, 6 months, and 1 year after the surgery. Additionally, all patients received a cervical spine magnetic resonance imaging (MRI) study prior to the surgery. The MRI study included T1-weighted and T2-weighted images with 3mm thin slices at sagittal, axial, coronal, and oblique sagittal planes perpendicular to the neuroforamen for evaluation. Post-operative MRI studies were performed at 3 months after the surgery. To evaluate facet preservation, we compared the pre-operative and post-operative axial MRI images using the method described by Matsumura et al. [24] and Dohzono et al. [25]. However, MRI was used instead of CT scan.
The independent t-test was used to compare continuous variables between groups, while the chi-square test was used to compare categorical variables. A p-value of <0.05 was considered statistically significant.
3. Surgical Techniques
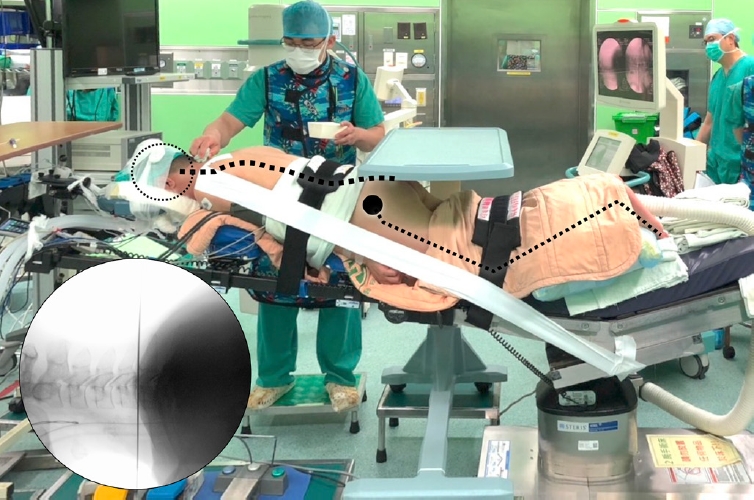
BEPCF is performed under endotracheal general anesthesia with the patient placed in a prone position on a radiolucent surgical table with his/her head supported by the headrest. The table must be adjusted to ensure free passage of the fluoroscope to obtain clear anteroposterior and lateral images. The patient’s shoulders are retracted caudally and fixed on the surgical table using adhesive tapes. The table can be tilted head-up or head-down to keep the segment of interest perpendicular to the floor for precise localization and more ergonomic handling of the endoscope and surgical instruments (Figure 1). Since the surgery is performed with continuous saline irrigation, a watertight draping is essential to prevent soaking and resultant hypothermia of the patient.
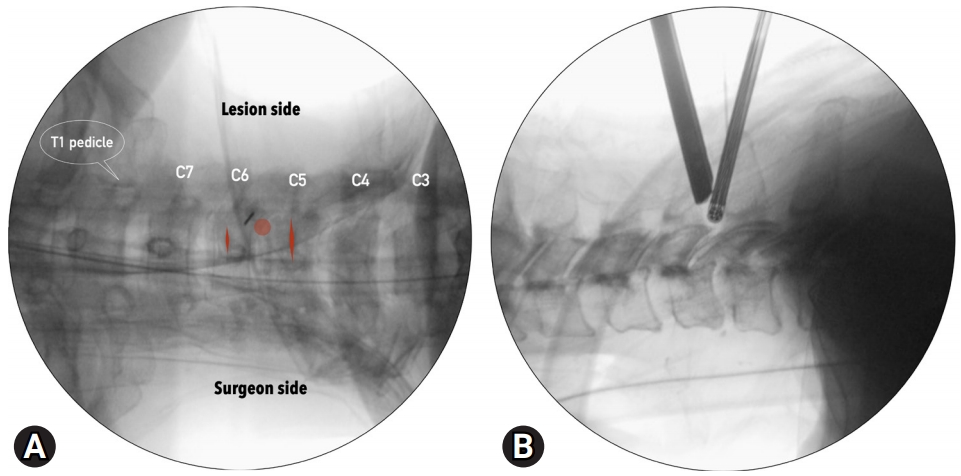
First, we determine the disc level of interest using the lateral fluoroscopic image. Then, using the anteroposterior images, we draw the skin markings. The V-point (junction of cranial and caudal laminae) must be clearly identified as the initial target for landing the endoscope and surgical instruments. For the contralateral inside-out approach, taking the left side foraminotomy for example, the surgeon stands on the patient’s right side, and the skin incisions are along the left lateral border of the spinous processes, separated by about 2 cm (Figure 2). For a two-segment decompression, a wider separation is needed.
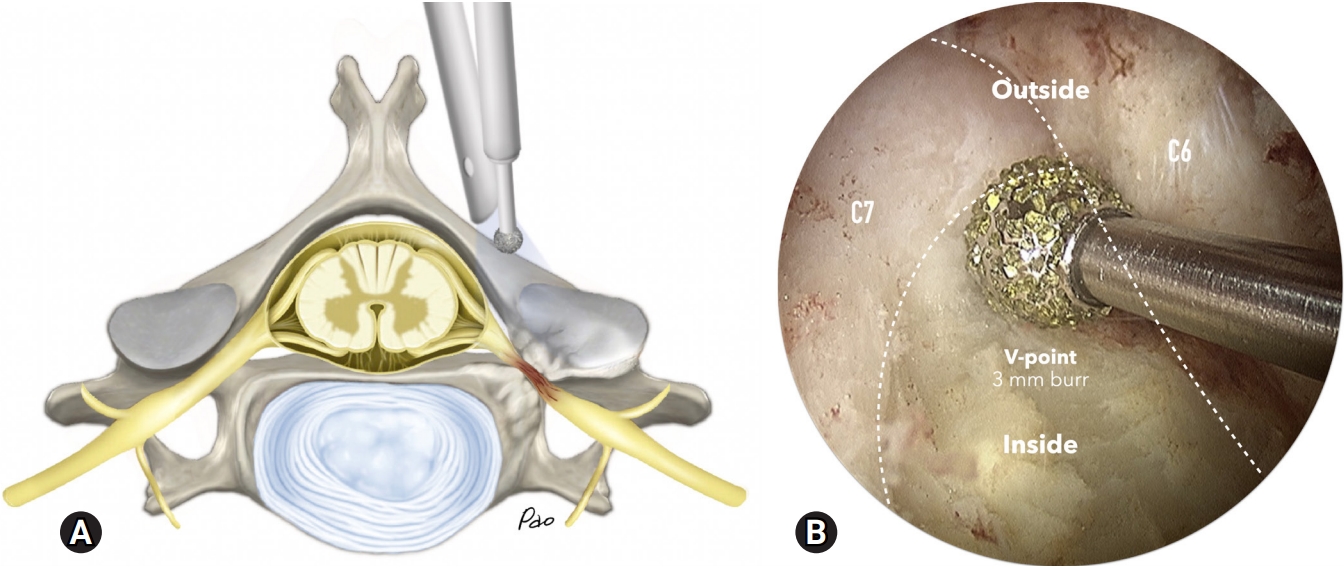
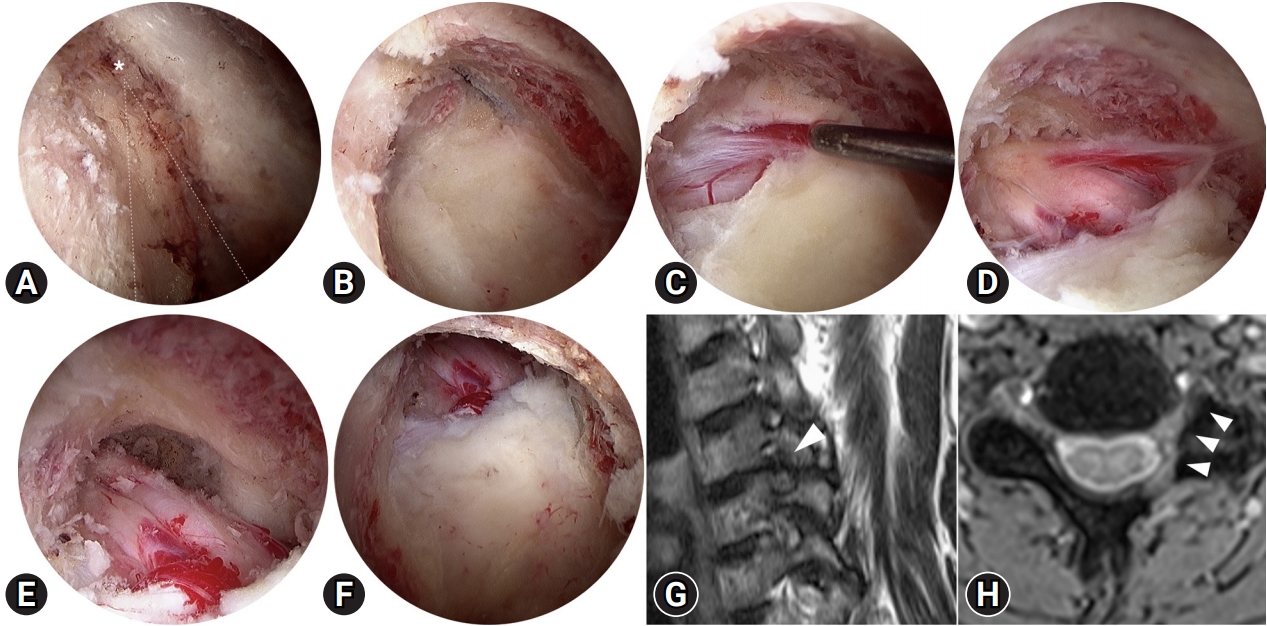
We prefer transverse skin incisions for better cosmetic results. The deep neck fascia is tough and requires a sharp No. 11 scalpel for penetration. Then, we use a blunt dilator to palpate the margins of the laminae around the V-point. The endoscope (4 mm ×30°; ConMed, Largo, Florida) and radiofrequency wand (ArthroCare, Austin, Texas) are inserted through independent skin incisions with inflow of normal saline. The triangulation formed by the endoscope, V-point, and radiofrequency wand must be confirmed under the fluoroscope (Figure 2). Use the radiofrequency wand to ablate the soft tissue to identify the V-point and create the working space required for the following procedures (Figure 3). Good control of saline inflow/outflow is mandatory to maintain a clear surgical field while using the high-speed drilling system.
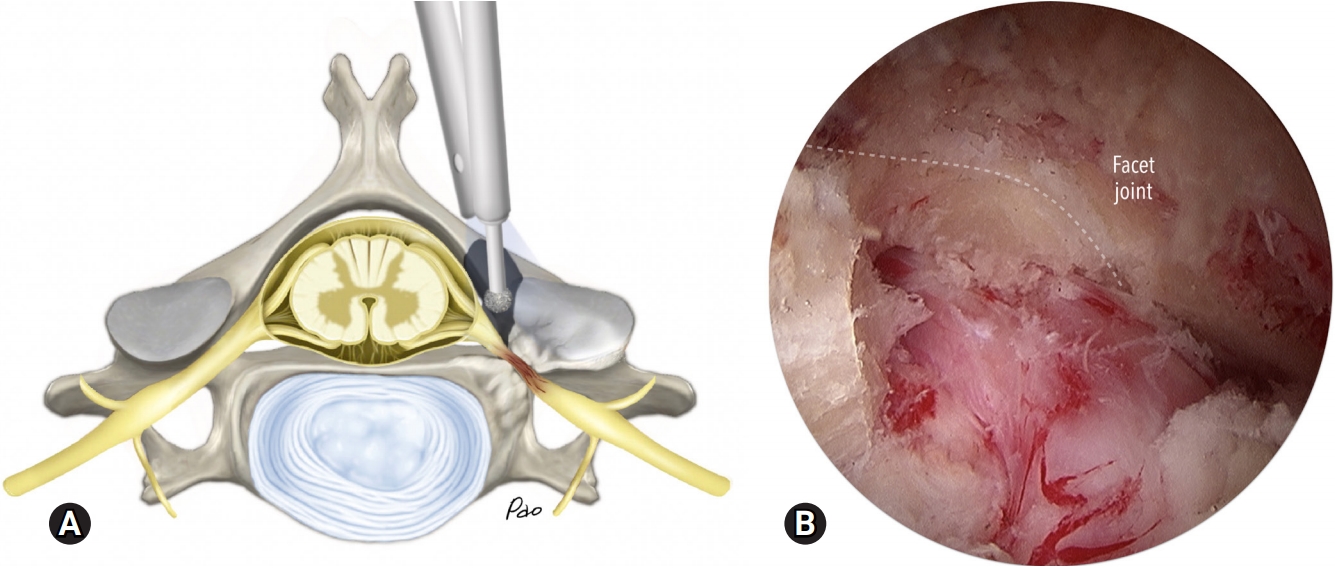
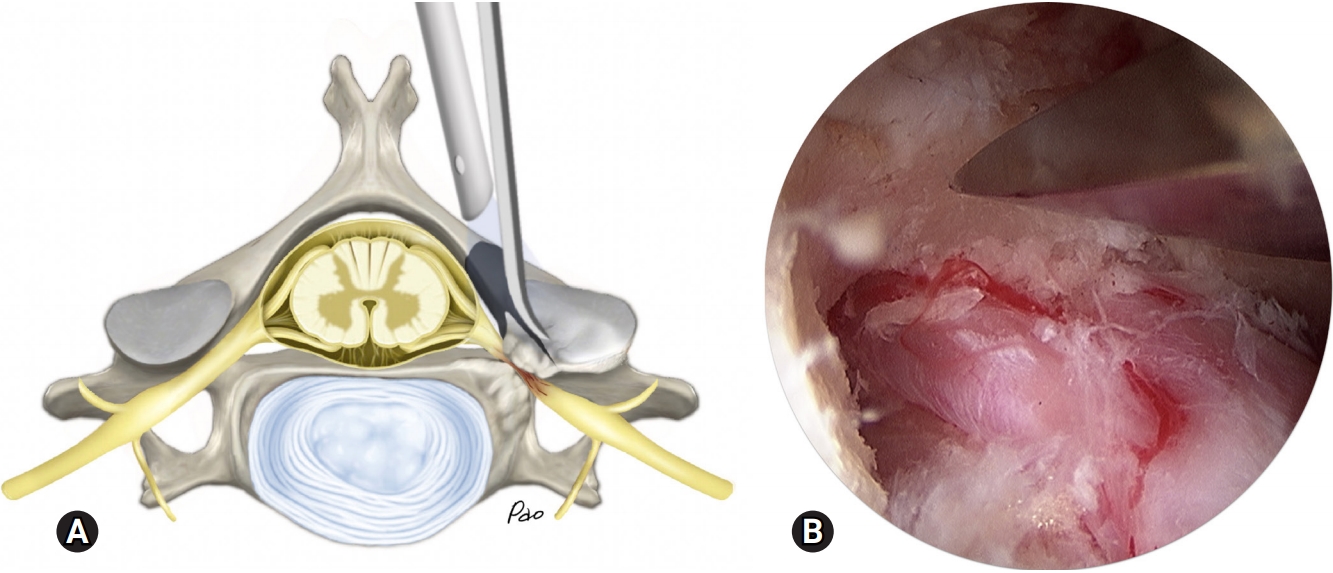
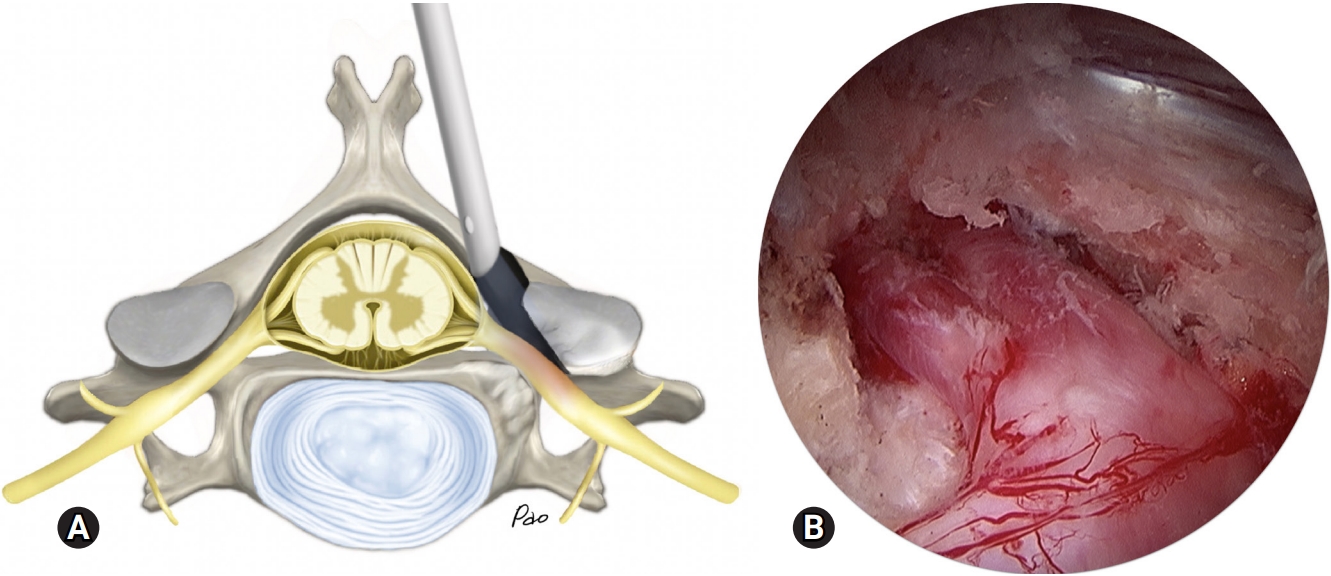
Starting from the V-point, extend the foraminotomy cranially, caudally, and laterally until the margin of the ligamentum flavum is exposed (Figure 4). A high-speed drill with a 3-mm coarse diamond ball tip (Primado II; NSK, Tokyo, Japan) is used as the primary instrument for removing bone. Use the nerve hook to elevate the ligamentum flavum and the underlying perineural membrane, removing only the portion of the ligamentum flavum which covers the nerve root. Coagulate the bleeders on the perineural membrane or epidural vessels using a 0.8 mm radiofrequency wand, and identify the nerve root. Use a 3-mm wide curved osteotome to undercut the cranial and caudal laminae to identify the inner surface of the pedicles. Then, use the same osteotome to undercut the superior articular process of the caudal vertebra (Figure 5). Use a small, angled curette to remove the bony fragments and free the nerve root. Check the adequacy of decompression and mobility of the nerve root using a nerve hook (Figure 6). Temporarily stop the irrigation to check the pulsation of the nerve root and identify the active bleeders. Use the radiofrequency wand to coagulate the bleeders and bone wax to seal the cancellous bone. Close the wounds by layers, using absorbable sutures to close the skin incisions and adhesive gel to secure them.
To control wound pain, the patient is given oral acetaminophen and intravenous morphine. They are allowed to ambulate with a soft neck collar. Typically, the patient is discharged from the hospital on the second postoperative day.
RESULTS
The average follow-up period was 15.5 months, ranging from 6 to 31 months. The average duration of hospitalization was 3.2±1.2 days, ranging from 2 to 6 days. The mean operation time was 58.4±15.4 minutes per segment of decompression (Table 1). Most patients experienced minimal pain at the surgical sites, and pain control with oral acetaminophen was usually sufficient. Only a few patients required one or two doses of morphine infusion. At the final follow-up, the VAS score for arm pain significantly improved from 7.3±2.2 to 0.9±0.7. The NDI also improved from 54.6±16.9 to 14.6±12.6. All these improvements were statistically significant from the baseline with p<0.005. According to the modified MacNab criteria, 21 patients (58.3%) had excellent results, 13 patients (36.1%) had good results, 2 patients (5.6%) had fair results, and no patient had poor results. The ratio of good and excellent results was 94.4% (Table 2).
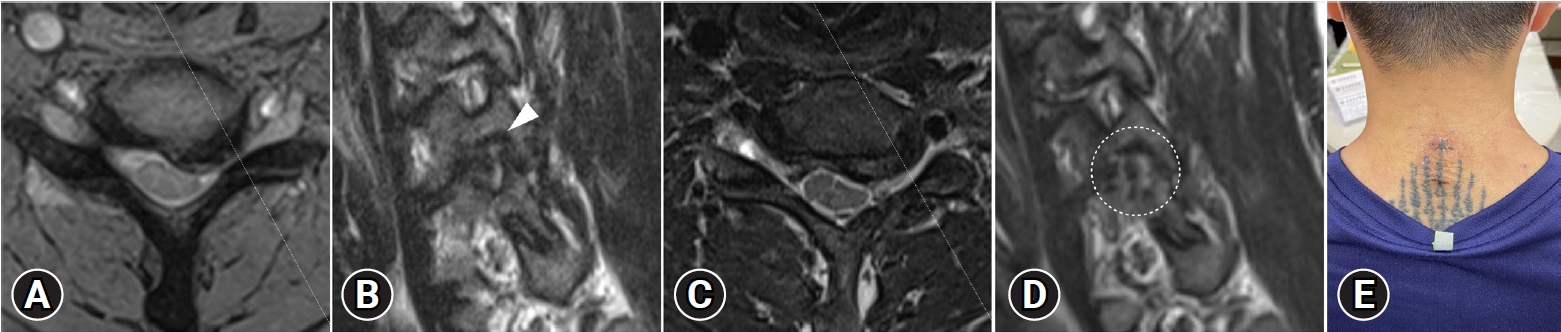
All patients underwent regular X-ray evaluations at 3, 6, and 12 months after surgery. We did not observe post-decompression segmental instability in any of our patients. Post-operative MRI follow-up at 3 months after surgery showed adequate decompression and enlargement of the neural foramen at the oblique sagittal plane with minimal facet joint destruction and soft tissue injury (Figure 7, 8). Post-operative MRI data were available for 22 patients, and the average facet preservation rate was 81.7%±8.0%, ranging from 64.5% to 91.5% (Figure 9).
Complications included two asymptomatic root abrasions and one case of transient neuralgia. There were no cases of dural tear or neurological complications. In the very early series, one patient experienced persistent radicular symptoms due to incomplete decompression. To alleviate his symptoms, a revision BEPCF procedure was performed (Table 1).
DISCUSSION
This study presents a minimally invasive surgical technique for treating cervical radiculopathy using the biportal endoscopic technique. The treatment resulted in good clinical outcomes, including significant improvement in VAS score and ODI, a short hospital stay, and a low complication rate. The contralateral inside-out approach provides adequate nerve root decompression with minimal facet joint destruction and soft tissue injury, while also offering ergonomic settings for the surgeon to perform the surgery.
The estimated annual incidence of cervical radiculopathy is 85 out of 100,000 people, and it usually occurs at the C5/6 and C6/7 levels [2,3]. The most common clinical presentations are radicular arm pain, followed by sensory deficit, neck pain, and reflex deficit [26]. Non-operative management, including medication, programmed rehabilitation, and epidural steroid injection, has been proven to achieve significant symptom relief in 75% to 90% of these patients [3,27]. However, for those who experience intolerable and persistent symptoms after conservative treatment, surgical decompression may be a good alternative solution. There are two mainstreams of surgical treatment: ACDF from an anterior approach, and PCF from a posterior approach [5,28].
ACDF removes the entire disc, restores disc height and lordotic alignment, and reconstructs segmental stability without damaging the posterior neck muscles. It is considered the gold standard surgical treatment for cervical radiculopathy due to its ability to provide quick and effective relief for neck pain, arm pain, and neurological symptoms [5,11,29]. However, there are many disadvantages associated with spinal fusion and the anterior approach that are also well documented in the literature [6-8].
In contrast, PCF decompresses the nerve roots directly via a posterior approach, avoiding the complications associated with an anterior approach. Several studies have shown that PCF provides comparable clinical outcomes in terms of symptom relief, complication rate, and patient satisfaction compared to ACDF, while preserving the range of motion of the cervical spine and avoiding adjacent segment degeneration [3,9,10]. A systematic review conducted by Liu et al. [11] summarizes that there was no significant difference in the complication rate and reoperation rate between ACDF and PCF within 2 years of the initial surgery. A meta-analysis conducted by Fang et al. [5] concludes that PCF is a sufficient alternative to ACDF with shorter operation time, shorter length of hospital stays, and a lower total hospital cost. However, the major drawbacks of traditional PCF are excessive damage to the posterior cervical musculo-ligamentous structures and destruction of the facet joints that contribute to segmental hypermobility and postoperative kyphosis [12,30,31].
To minimize soft tissue damage in open surgeries, a minimally invasive approach using the tubular retractor has been adopted since Dr. Foley and Smith [32] introduced the concept of microendoscopic surgeries in 1997 [33,34]. The microendoscopic PCF shares the advantages of traditional PCF but minimizes iatrogenic damage and has been reported to provide comparable results in clinical outcomes [28,35,36]. However, handling surgical instruments to perform delicate procedures in such a small tubular retractor is challenging. Even with the assistance of a specially designed endoscope or microscope, it still requires a steep learning curve to achieve stable treatment results and reduce the possibility of neurological complications [37].
In this study, we introduce a contralateral inside-out PCF technique using biportal endoscopy to treat cervical radiculopathy. Compared to traditional microscopic or microendoscopic PCF, the biportal endoscopic approach results in an almost bloodless surgical field. Normal saline is used to provide hydrostatic pressure to suppress bleeding and carry away bone debris. Although the working space may be small, a high-resolution 30-degree endoscope provides a clear, bright, wide, and magnified surgical field of view [38-40]. The operator and assistants perform the procedure on a video monitor, eliminating the need to bend their necks or strain their eyes on a microscope. The operator holds the endoscope in one hand and surgical instruments in the other, allowing for a relaxed neck and shoulder posture and minimizing the risk of neurological complications during delicate surgical procedures.
Biportal endoscopic surgery has been successfully used to treat a variety of degenerative conditions in the lumbar spine [16-21]. Several studies have shown that the clinical outcomes of biportal endoscopic surgeries are comparable to those of microscopic or microendoscopic approaches [41-44]. A comparative study of three types of minimally invasive decompressive surgery in patients with lumbar spinal stenosis was conducted by Heo et al. [41]. The study showed that the endoscopy groups, either uniportal or biportal, had better clinical outcomes in the immediate postoperative period than the microscopy group. The better outcomes were possibly due to less soft tissue injury related to surgery in the endoscopy group [41]. Our study also showed that BEPCF is very effective in relieving preoperative arm pain and neurological symptoms, with minimal pain from the surgical sites.
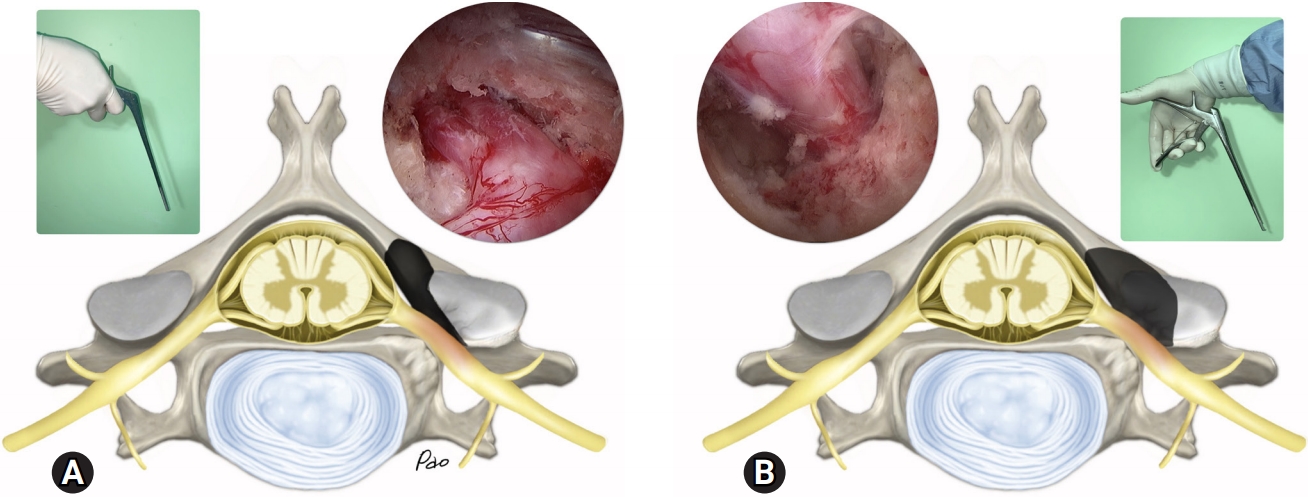
The contralateral inside-out approach differs significantly from the ipsilateral approach (Figure 10). Although the decompression of the nerve root may be equally effective with both approaches, the extent of laminotomy required to achieve an effective decompression is much smaller with the contralateral inside-out approach. Consequently, there is less facet joint destruction. By undercutting the superior articular process, the contralateral inside-out approach may preserve a greater proportion of the facet joint and capsule [45,46]. Therefore, the contralateral inside-out approach may reduce the risk of post-decompression segmental instability or progressive kyphosis after the surgery [14,15]. However, this theoretical advantage requires a long-term follow-up study to validate.
Handling of the endoscope and surgical instruments is more ergonomic for the contralateral inside-out approach. With the surgeon positioned on the contralateral side, the endoscopic viewpoint naturally follows the direction of the nerve root from its origin to beyond the foramen. Additionally, handling surgical instruments aligns with the natural posture of the hand. Conversely, the ipsilateral approach presents the endoscopic viewpoint from the opposite side, forcing the surgeon to handle surgical instruments in a non-ergonomic, reversed manner.
The current study has several limitations. First, it is a retrospective study with a small sample size and short-term follow-up. Second, all surgeries were performed by a single spine surgeon who is experienced in minimally invasive and endoscopic spine surgeries. The treatment results and complications may differ if surgeries are performed by another surgeon with a different level of experience. Third, long-term or comparative studies are needed to verify the theoretical or proposed advantages of the contralateral inside-out BEPCF.
CONCLUSION
BEPCF is a simple, effective, and safe minimally invasive surgical technique for treating unilateral cervical radiculopathy. With appropriate patient selection, spinal fusions and their associated negative consequences can be avoided. When BEPCF is done via the contralateral inside-out approach, the surgeon can perform an effective decompression in an ergonomic setting while preserving the facet joint.