INTRODUCTION
Transforaminal lumbar interbody fusion (TLIF) has been regarded as gold standard for lumbar fusion providing effective decompression of neural tissue while avoiding neural injury. Open spine procedures though address the pathology, is known for prolonged duration of anesthesia, blood loss, delayed recovery of the paraspinal muscle injury, prolong hospital stay leading to increased costs. With advancement in technology, more efficient techniques such as minimally invasive TLIF have become popular. However, mis TLIF still requires considerable length of incision and damage to musculature due to long tubular retractors also causing difficulty to work in depth with limited working space [1]. Advancement in endoscopic techniques have further revolutionized minimally invasive spine surgery resulting in minimal blood loss, decreased soft tissue destruction, minimal post-operative pain and faster recovery [2]. Transforaminal (Trans Kambian) endoscopic approach has the advantage of reaching intervertebral foramina and the disc directly, achieving decompression and fusion without excision of lamina, inferior and superior articular process, and ligamentum flavum [3]. However, foramen and lateral recess can be decompressed thoroughly, endoscopically if required. Visualized endplate preparation done as in our technique ensures improved fusion rates.
CASE REPORT
History
A 30-year male, came with history of fall of heavy metal pipe on his lower back while working. He presented with severe lower back pain (VAS score 9/10), right lower limb radiculopathy (VAS 8/10) with numbness in calf and dorsum of foot.
Examination
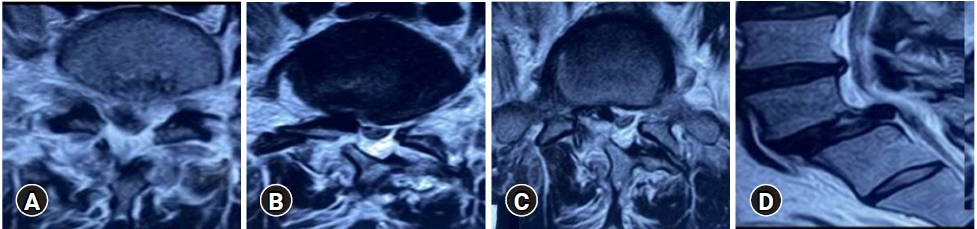
Clinical examination revealed a palpable step off at L5-S1 with severe touch and pressure tenderness. Straight leg raising test was positive on right side (20°). Further examination revealed decreased sensation over right dorsum of foot with no motor deficits. Magnetic resonance imaging of lumbo-sacral spine was suggestive of L5-S1 Grade 1 spondylolisthesis with bilateral pars fracture with disc herniation compressing right S1 nerve root (Figure 1).
CT lumbosacral spine confirmed L5-S1 Grade I spondylolisthesis with bilateral pars interarticularis fracture with intact pedicles (Figure 2).
With written and informed consent patient underwent Transforaminal (Trans Kambian) Endofusion with removal of disc fragment under epidural analgesia and continuous intraoperative nerve root monitoring.
Surgical method
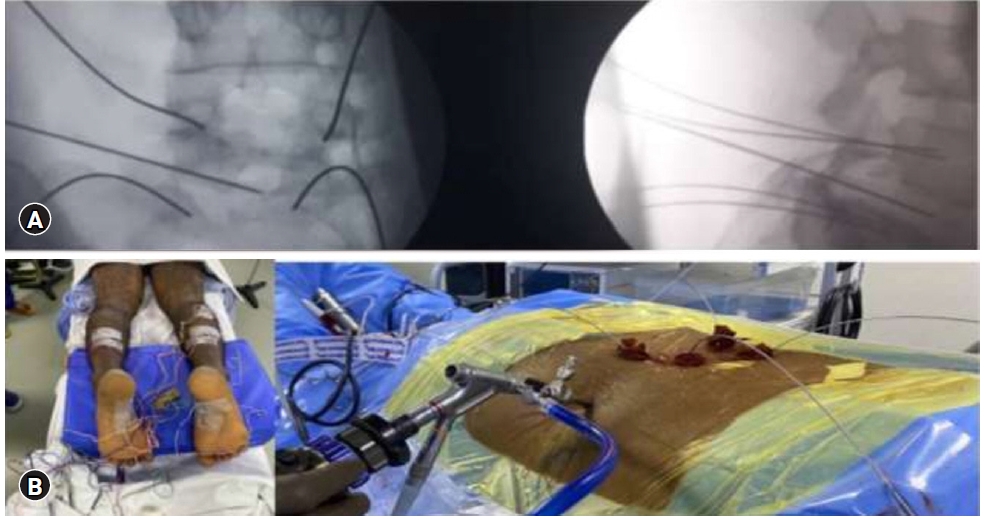
Patient was placed on comfortable bolsters in prone position after Epidural catheter was placed in L1-L2 space and analgesic dose of ropivacaine was given. Nerve monitoring using raw EMG’S and triggered EMG’S were applied in both lower limbs. After cleaning and draping L5-S1 pedicles were entered percutanously using Jamshidi needles under fluoroscopic guidance bilaterally (Figure 3).
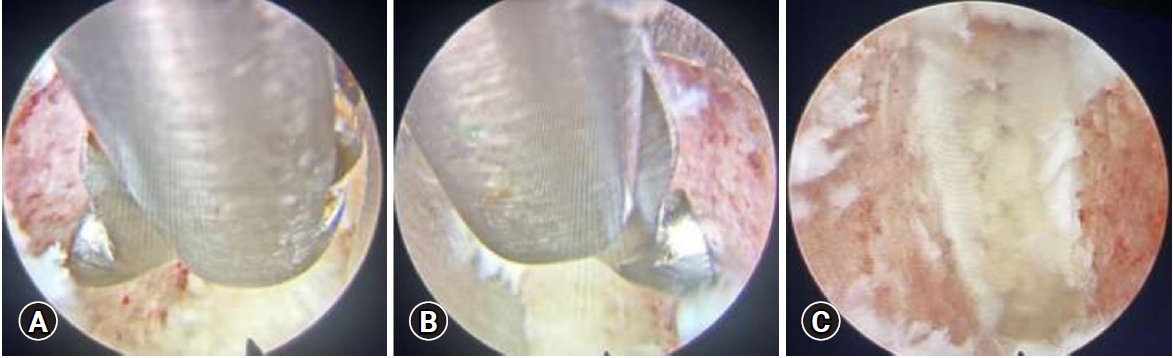
Guidewires were secured bilaterally and position confirmed both in AP and Lateral views. Using C-arm AP/Lateral entry point was marked at L5-S1 level, 10 cm from midline. Local anesthetic infiltration (Lignocaine) was given. 18-gauge, 20 cm spinal needle guided under antero-posterior and lateral fluoroscopy, to access the disc space transforaminally via Kambin’s triangle at L5-S1 level. Care was taken to ensure the trajectory of the needle was such that the eventual placement of the interbody device was central in antero-posterior view, and anterior in the lateral projection. A guide wire was introduced through the needle, into the disc space, after the removal of stylet. Tapered dilator was advanced over the guide wire and docked into the disc. A bevel-ended working cannula was introduced over the dilator. The guidewire and dilator were withdrawn, and a 4.1mm working channel endoscope was inserted through the cannula. Discectomy and endplate preparation for interbody fusion were performed using a combination of Disc forceps, specially designed articulating curettes and 4MHz RF through the endoscopic channel visualizing throughout while preparing the endplates with removal of disc and endplate cartilage (Figure 4).
Endoscopic visualization ensured the adequacy of end plate preparation, which was confirmed by visualization of the subchondral bone and petechial bleeding. Care was taken to preserve the subchondral bone to minimize the risk of subsidence of interbody cage. Following endplate preparation, ChronOs (Depuy synthes) mixed with bone marrow aspirate, which was obtained from the iliac crest (Figure 5), was packed anteriorly in the disc space through the working cannula. Once the fusion site preparation was done, endoscopic system was withdrawn with guidewire in situ and the specially designed (11×30 mm Titanium) Interbody fusion cage was inserted over the guidewire under fluoroscopic guidance, with neuromonitoring confirmation. Guidewire was removed after position of cage was confirmed on C-arm. Percutaneous Pedicle screws were then inserted bilaterally and connecting rods were placed (Figure 6).
Outcome
In the immediate post-operative period patient had significant relief in both back and leg pain (VAS 2/10). Patient was mobilized as per pain tolerance and was discharged within 24 hours of the procedure with minimal analgesics. Immediate postoperative CT Lumbo Sacral spine scan confirmed complete reduction of listhesis with satisfactory position of cage and pedicle screws in situ.
DISCUSSION
Lumbar spine fusion has come a long way since Cloward had described Posterior Lumbar Interbody Fusion (PLIF) in 1943 [4]. Although PLIF is still performed, many surgeons prefer Transforaminal Lumbar interbody Fusion (TLIF) pioneered by Harms and Rolinger in 1982 which has significant advantages over PLIF [5]. Open spine procedures though address the pathology, is known for prolonged duration of anesthesia, blood loss, delayed recovery of the paraspinal muscle injury, prolong hospital stay leading to increased costs, Persistent back pain due to para spinal muscle damage. Use of minimal invasive lumbar interbody fusion has been increasingly popular method of lumbar arthrodesis, in an attempt to decrease operative morbidity, ever since minimally invasive TLIF has been described by Foley et al. [2]. Enhanced recovery after surgery has been attempted in field of spine surgery ever since Wang et al. [6] introduced emphasizing importance of endoscopic lumbar interbody fusion. They aimed at reduction in operative scars and traumatization of posterior musculoligamentous structures.
Endo-TLIF provides significant advantages over minimally invasive and open TLIF. Endo-TLIF provides a better alternative technique than conventional procedures for the case discussed above (traumatic lumbar listhesis) minimizing muscle trauma in an already injured patient.
Following advantages were noticed in our case over conventional surgery.
Endoscopic TLIF was done under epidural analgesia giving it an advantage over general anesthesia [7] such as fewer parental narcotics, lower incidence of urinary retention, accessibility of verbal interaction between the surgeon and patient helping in intraoperative assessment by facilitating real-time neurological feedback from the patient, fewer episodes of hypertension intraoperatively and is much more feasible for patients having comorbidities. In our case ropivacaine was used for epidural analgesia in the present case.
Although studies have suggested end plate preparation to be equivalent in minimally invasive TLIF and open TLIF [8], endplate preparation is better in Endo TLIF as it is done under direct vision removing the disc material and endplate cartilage without injuring the subchondral bone.
Smaller surgical scar, minimal blood loss, no muscle retraction are other advantages seen in endo TLIF technique. Use of nerve monitoring helps in avoiding any neurological deficit intraoperatively.
Osman [9] concluded in their Endofusion series, that the endoscopic transforaminal lumbar decompression, interbody fusion consistently produced satisfactory results and it performed better than the alternative surgical options studied.
Overall hospitalization time for Endo TLIF is significantly less resulting lesser cost of treatment. Decrease in surgical time and tissue disruption, minimal postoperative pain and nausea significantly aid in reducing patients’ recovery period and analgesia [10]. In present case patient was mobilized and discharged on the same day of surgery.
CONCLUSION
Endo-TLIF is an effective and safe, least invasive surgical option for interbody lumbar fusion when chosen wisely. To our knowledge ours is the first case to be reported in the literature of traumatic bilateral pars fracture treated with Endo-TLIF. Indication of Endo-TLIF can also be extended to cases of traumatic pars fractures with or without spondylolisthesis.