INTRODUCTION
Minimally invasive spine surgery (MISS) techniques for lumbar spine pathologies are very frequently performed in recent days. MISS techniques are associated with reduced blood loss, faster recovery and reduced postoperative morbidity while yielding similar results to open procedures [1-4]. MISS provides a narrow corridor to the spine and results in minimal tissue injury. The microendoscopic approach in lumbar spine surgery for the treatment of prolapsed intervertebral disc (PIVD) was reported by Perez-Cruet et al. [5] in 2002, following Foley and Smith’s description in 1997 [6]. Non expandable tubular retractor systems are commonly used for MISS technique lumbar spine surgery, with the tubular retractor system we can approach the spine with minimal muscle dissection and cosmetic appealing incisions, which results in decreased postoperative surgical site pain and faster recovery after surgery. Microendoscopic discectomy (MED) and minimally invasive lumbar canal decompression are the most frequently performed surgeries using tubular retractor system. Accidental durotomies (ADT) are undesirable but frequent intraoperative complications. Current review of literature says the frequency of ADT in MISS is reported to range from 3.2% to 16.7% [7,8]. Once a dural tear has occurred primary repair is difficult due to limited surgical field. Intraoperative management of an accidental durotomy, with leakage of cerebrospinal fluid (CSF), includes sealing the leakage of fluid from the intradural space. This is usually accomplished by direct suture of the dural tear, applying a sealant or combination of these modalities. Diversion of CSF flow from the durotomy by placement of lumbar drain is sometimes performed. Some surgeons also routinely place a subcutaneous drain [9]. We studied the incidence of ADT in MED and minimally invasive lumbar spine decompression surgeries, intraoperative management, complications, its impact on the surgical outcomes and the mobilization protocol of the same patients. In addition, we analyzed the risk factors related to dural tears in these surgeries.
MATERIALS AND METHODS
After receiving an approval from the local medical council ethical committee, we prospectively studied 550 patients from January 2012 to March 2020 who underwent MED and minimally invasive lumbar decompression surgeries in single institution by single surgeon. Patients presenting with neurogenic claudication and/or radicular symptoms in the lower limb either due to lumbar prolapsed intervertebral disc (PIVD) and/or lumbar canal stenosis (LCS) at the lumbar spine levels (L3-4, L4-5, L5-S1) lasting for more than six to eight weeks and who failed to respond to conservative mode of management (with bed rest, painkillers and/or epidural steroid injections) where included for the procedure. Patients with a recurrent disc herniation with or without radicular symptoms who had undergone same level surgery previously, patients who needed greater than 2 level decompression, patient with intervertebral instability (>25% intervertebral slip, >4 mm translation) on flexion and extension, upright lateral radiographs were excluded from the study. We performed a lumbar MED using tubular retractor systems for patients with lumbar PIVD using unilateral approach and for patients with lumbar canal stenosis we additionally performed a bilateral decompression using a unilateral approach. We noted patients demographic data like age, gender, height, weight, smoking status and presence of diabetes. Type of procedure and occurance of accidental duratomies were recorded. We analysed if age, body mass index (BMI), smoking, diabetes had a significant influence on the incidence of ADT. As per age patients were divided into 3 cohorts, 20–40 years, 40–60 years, and >60 years. A standard three sample test for equality of proportions was performed considering the ADT rates within the three groups. For BMI, Cohorts were made according to the WHO classification. BMI was calculated by dividing the subjects mass in kilograms (kg) by the square of the persons height in meters (BMI=kg/m2). Patients with BMI<25 are normal weight, BMI>25 and <30 as overweight and those with BMI>30 obese. Testing for the significant differences between the BMI groups was performed using a standard three sample test for equal proportions. Testing of significant difference in between diabetics and non diabetics, smoker vs. non-smokers was performed using standard two sample test for equality of proportions.
1. Surgical Technique
All surgeries were performed under spinal anaesthesia. Patients were positioned on a radiolucent table in prone position with bolsters underneath to keep the abdomen free, head end raised and pressure points well padded. Surgeon stood on the side with dominant lower limb radicular symptoms. Under fluoroscopic guidance the lumbar spine level to be operated was identified and surface marking done. Under fluoroscopic guidance an 18-guage spinal needle placed at the spinolaminar junction of the same level to be operated. Normal saline injected to make a tract in the subcutaneous and muscular plane. 20–22 mm vertical paracentral incision taken 1 cm lateral to the midline. Subcutaneous tissue and fascia incised in the line with the skin incision. Sequential dilation done using dilators of the tubular retractor system and a 22 mm tube final docking done. In patients with paracentral disc prolapse and/or unilateral lower limb radiculopathy, unilateral laminotomy, flavectomy followed by removal of the herniated disc fragment was done. In patients with lumbar canal stenosis and/or bilateral lower limb radiculopathy, the tubular retractor was tilted medially and patient along with the operating table rotated away from the surgeon side and microscope adjusted to visualize the under surface of the spinous process, undercutting of the spinous process and contralateral lamina and contralateral flavectomy done to complete the bilateral decompression. Any disruption in the dural integrity with or without CSF leak recognized during the surgery is considered as dural tear. In patients with accidental duratomies and CSF leak, the CSF leak was controlled using gelfoam/fibrin glue as an onlay technique. Primary repair of the dura was not done neither was any drain placed in cases of accidental duratomies. The retractor system removed and in cases with no dural tear the wound closure consisted of approximation of lumbar fascia and subcutaneous tissue with absorbable suture material and skin closure with absorbable monocryl suture and in cases with dural tear the lumbar fascia and subcutaneous tissue approximated in the same fashion but the skin was closed in a water tight fashion using nonabsorbable ethilon sutures. The occurance and details including the type of dural tear were recorded at the time of the surgery by the attending surgeon. Patients were followed up for a minimum of 1 year after surgery, during which patients underwent clinical evaluation and MRI at 6 months interval. The clinical outcome was assessed using the modified Oswestry disability index (ODI) and Japanese Orthopaedic Association (JOA) scores for the management of low back pain [10]. Improvement in the ODI score was calculated by substracting pre- and postoperative ODI score and improvement in JOA score were evaluated by Hirabayushi’s method [11].
2. Postoperative Mobilization Protocol
All patients were operated under spinal anaesthesia, so patients were awake and alert postsurgery and were directly shifted to respective wards with head of bed (HOB) at zero position. Patients with no dural tear were allowed to sit bedside and mobilized bed side 4–5 hours postoperatively once the effect of spinal anaesthesia has completely wained off. In patients with intraoperative dural tear the head end was gradually elevated to 45 degree once the effect of spinal anaesthesia is wained off and monitored for any symptoms of intracranial hypotension (ICH) like headache, nausea for 4–5 hours and if no symptoms the patients were mobilized on postoperative day 1 and if symptoms present then the patients were instructed to keep HOB at zero position until next morning and whole postoperative day 1. They were allowed to sit up in bed for diet and to ambulate for bathroom usage. Postoperative day 2 patients were revaluated and if symptoms of ICH relieved then patient mobilized and discharged, if symptoms persists patient discharged with advice of HOB at zero and limited mobilization protocol till symptoms subsides and were followed with daily teleconsultation services. Occurance of postoperative dural tear complications like ICH symptoms, meningitis, psuedomeningocele were noted.
3. Statistical Analysis
Data were analysed using IBM SPSS statistics version 22. All continuous variables were found to be normally distributed using the Kolmogorov-Smirnov test, which allowed for parametric testing. Normally distributed data were compared using Student’s t-test. Nominal data were compared using the chi-squared test, and p<0.05 was considered statistically significant in order to identify risk factors associated with accidental durotomies.
RESULTS
Study conducted over a period of 8 years, with 550 consecutive patients which included 320 males and 230 females who underwent MED and minimally invasive lumbar decompression and patient demographics were noted (Table 1).
1. Incidence of Accidental Durotomies and Risk Factors
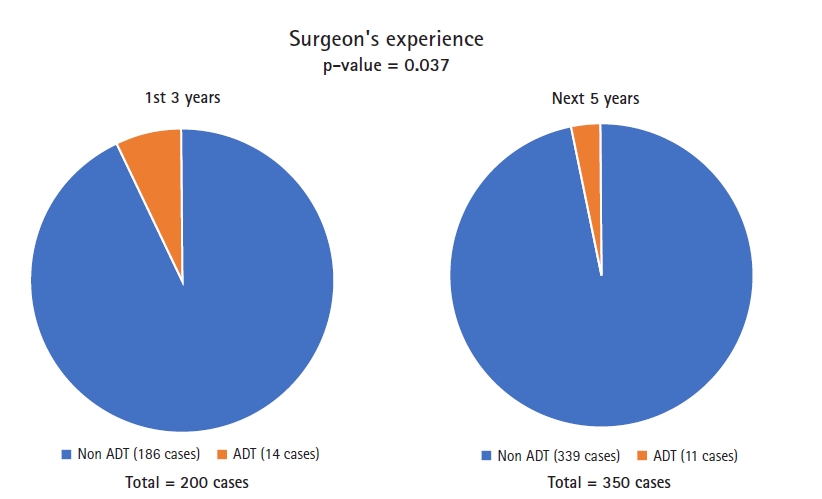
A total of 25 patients (14 male, 11 female; 4.54%) had intraoperative dural tear. The mean age of these patients was 56.15 years (24–86 years). Patients of age above 60 years had significantly higher dural tears than those below 60 years p-value=0.0062 (Table 2). There was no statistical difference in gender between the groups. There was no significant difference in the rate dural tears between smokers and non smokers and neither with diabetics and non diabetics (Table 3, 4). The technique of BLD had statistically significant higher rates of dural tears when compared to ULD both in the initial 3 years and next 5 years with p-value of 0.032 and 0.016, respectively. Among the three BMI groups there was significant difference the incidence of dural tears. Out of the total 200 patients operated in the initial 3 years 14 patients suffered ADT (7%) and in the next 5 years out 350 operated patients 11 had ADT (3.14%), showing a significant fall in the incidence of ADT with improvement in surgeons surgical experience (Figure 1).
2. Accidental Durotomies and Clinical Outcome
All the 25 patients with dural tear were managed intraoperatively using sealants like subcutaneous fat, gelfoam and fibrin glue. Primary repair of the dural tear was not done in any of the patients. Only 2 patients with ADT had symptoms of ICH which subsided within 2 postoperative days, it was also noted that among the other 525 patients 12 patients had symptoms of ICH without ADT probably due to the needle puncture that occurred during administration of spinal anaesthesia (Table 5). None of the patients developed meningitis nor pseudomeningocele in 6 month follow-up MRI. Postoperatively patients were assessed with modified Japanese association score recovery rate and were 73.8% and 76.3% among patients with ADT and patients without ADT respectively, improvement in the ODI score were also noted which was 39.5 and 37.5, respectively in ADT and non ADT patients. No statistically significant difference in the recovery rate of m JOA and improvement range of ODI was noted in the 2 groups.
DISCUSSION
Accidental duratomies are frequent intraoperative complications in lumbar spine surgery. As per the literature the incidence is around 9% to 14% in open lumbar surgeries [7,8], 6.3% in MISS procedure [12]. In our study which included 550 patients total 25 patients (4.54%) had intraoperative dural tear. The prospective design and large sample size were the strength of the study. In our study we noted that incidence of ADT significantly reduced in the later 5 years of the study than the initial 3 years showing that the surgeons experience plays a major role in incidence of ADT. Lack of stereoscopic vision and poor depth perception in the initial days of surgeons practice might be one of the reason for higher incidence of ADT [13,14], indicating a steep learning curve to master the technique. We analysed some of the readily available parameters like age, BMI, smoking status and diabetes mellitus (DM). Increasing age had a significant correlation with the incidence of dural tear, probably due to thin duramater caused by ageing and frequent adhesions seen between the duramatar and surrounding tissue in elderly patients with LCS. With the ageing process the yellow ligament degeneration increases and its elasticity is lost, resulting in the deposition of calcium crystals in the yellow ligament during the bone formation process leading to its ossification [15]. Epstein [7] found a marked association between these ossified yellow ligament and ADT. In our study we noted that dural tear mainly occurred during contralateral decompression specifically while undercutting the spinous process and during contralateral laminotomy and flavectomy which can be explained because of the loss of elasticity of the flavum and adhesions between the dura and flavum and also the surgical expertise required. It is a well known fact that smoking and DM lead to poor outcomes after spine surgery because of increased risk of surgical site infections, wound healing disorders and more reoperations [16,17]. DM is a known non-genetic risk factor in the pathophysiology of ossification of posterior longitudinal ligament (OPLL) [18], but the role of both smoking and DM in the degeneration of ligamentum flavum is not well studied. In our study the correlation between smoking and DM with the incidence of ADT was statistically insignificant. Cole and Jackson [19] performed minimally invasive lumbar discectomies in 32 obese patients, ADT were the most common complication at a rate of 9.4% and they concluded that the higher rate of ADT was related to the longer working area in the obese patients. In contrast we found no significant correlation between ADT and all 3 BMI groups. Our experience during the course of the study was that a minimal invasive technique using tubular retractors and microscopic enhanced vision avoids difficult dissection through the fat plane in open surgery and gives a precise working field and clear distinction of tissues due to enhanced microscopic vision. We recommend a minimal invasive technique for spine surgery over open technique in obese patients. Accidental durotomies can lead to persistant CSF leakage leading to formation of CSF fistula, pseudomeningocele, symptoms of ICH like nausea and postural headache, back pain, intracranial hemorrhage and meningitis [20,21]. Most of the authors agree that the dural tear has to be repaired primarly [22]. But small working space available by using tubular retractor system in MISS makes the primary dural repair difficult. In our study we noted that most of the dural tear were small and could be managed with overlay sealants like subcutaneous fat, fibrin glue, gelfoam. All 25 patients who suffered ADT were managed intraoperatively using fibrin glue and gel foam no primary dural repair done. We also found that some of the patients without intraoperative ADT also developed ICH symptoms which explained due to needle puncture during the administration of spinal anaesthesia (SA). Thus even if ADT does occur in MISS, it is less likely to cause sequelae because in the MISS surgical approach the paraspinal muscles are not dissected and they slip back to their original position once the tubular retractor system is removed resulting in minimal dead space available for CSF accumulation thus preventing the formation of CSF fistula and pseudomeningocele [12,23]. We agree with authors [12,20] and do not use drain in MISS. Early mobilization is recomemded in elective spine surgery to avoid complications like venous thromboembolism [24]. We mobilized all are patients including the patients with ADT and no ICH symtoms on postoperative day 1 and maximum postoperative day 2 for patients with ADT and ICH symptoms. Very few patients required HOB at zero and limited mobilization till postoperative day 3. We therefore agree with Ruban and O’Toole [20] and Than et al. [12] for within 24 hours early mobilization protocol after MISS. This early mobilization protocol prevents postoperative deep venous thrombosis and reduces the length of hospital stay.
CONCLUSION
MISS has low incidence of ADT and age >60 years and surgical technique of bilateral decompression with unilateral approach and surgeons expertise are the significant risk factors. MISS also has less risk of CSF leak symptoms and pseudomeningocele formation because of limited dead space formation in the soft tissue which inturn helps in early postoperative mobilization and reduces the duration of hospital stay.