The Significance of Lumbar Probing Combined with Continuous Irrigation and Undercutting Posterior Vertebral Body for Highly Upward Migrated Disc Herniation in ACDF: Case Reports and technical notes
Article information
Abstract
The purpose of this report was to present successful cases and technical notes of the patients with up migrated cervical disc herniation to the upper level who were successfully treated using anterior cervical discectomy and fusion (ACDF), describing the evaluation of treatment outcomes and perioperative complications. The cases of two patients who had ACDF in symptomatic up migrated cervical disc herniation to the upper level in February 2021 and November 2021 were reviewed. Two patients presented with a six-week history of posterior neck pain and radiating pain. Preoperative magnetic resonance imaging (MRI) confirmed a diagnosis of up migrated cervical disc extrusion. The patients were admitted to Daegu Wooridul Spine Hospital in Daegu, Korea. ACDF was performed under general anesthesia. Treatment outcomes were examined by comparing pre and postoperative Numeric Rating Scale (NRS), and MRI. Treatment outcomes were favorable: posterior neck pain and radiating pain showed a significant reduction in NRS. Postoperative MRI showed that the up migrated discs were successfully removed in both cases. Neither patient developed perioperative complications. Anterior cervical discectomy can be feasible in patients with symptomatic up migrated cervical disc herniation to the upper level.
INTRODUCTION
Highly migrated cervical disc extrusion is rare [1]. Disc fragments can migrate upward or downward. Migrated disc fragments in the cervical spine are classified into four types according to their locations on the anterior, lateral, and posterior surface of the dural tube [2]. Most of the migrated disc fragments are located on the anterior or lateral surface of the dural sac, which can lead to myelopathy or radiculopathy.
Symptomatic up migrated cervical disc herniation necessitates surgery. If disc sequestrations are located on the anterior or lateral surface of the dural tube, the anterior approach is considered an effective way to decompress the cervical cord and nerve root [2]. The use of corpectomy rather than discectomy for up migrated cervical disc herniation to the upper level was advocated [1,2]. However, compared to anterior cervical corpectomy and fusion (ACCF), anterior cervical discectomy and fusion (ACDF) may lessen the scarification of normal disc level and cervical motion, as well as the rate of adjacent segment disease (ASD) [3]. Therefore, if ACDF is feasible and successful in up migrated cervical disc herniation to the upper level, ACDF will be more beneficial to the patients compared with ACCF.
In this report, we present two cases of patients with up migrated cervical disc herniation to the upper level behind the vertebral body. ACDF was performed using exploration of up migrated disc combined with continuous irrigation and undercutting posterior vertebral body. Treatment outcomes were favorable, with no perioperative complications.
CASE REPORT
1. Case 1
In February 2021, a 45-year-old man complained of severe posterior neck pain and right radiating pain six weeks ago, for which he was admitted to the Daegu Wooridul Spine Hospital in Daegu, Korea. The patient’s Numeric Rating Scale (NRS) was 8 [4]. He had difficulty moving his neck posteriorly. Preoperative magnetic resonance imaging (MRI) and computed tomography (CT) showed non-calcified cervical disc extrusion with up migration on C3-4, C4-5 (Figure 1).
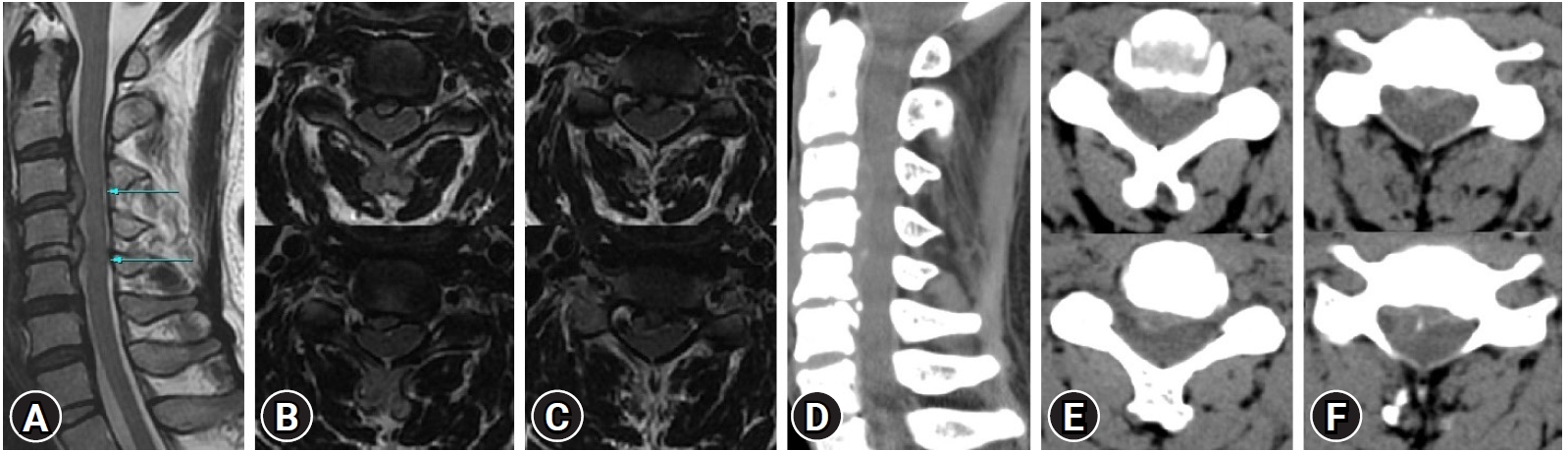
Preoperative images of the up migrated cervical disc herniation at C3-4, C4-5 level on MRI and CT. (A) A mid-sagittal image on T2 weighted MRI. (B) Axial images at C3-4 level on T2 weighted MRI. (C) Axial images at C4-5 level on T2 weighted MRI. (D) Mid-sagittal images on CT. (E) Axial images at C3-4 level on CT. (F) Axial images at C4-5 level on CT.
After informed consent was obtained from the patient, ACDF was performed in February 2021. 5 mm high PEEK cages on C3-4, C4-5 and an anterior plate were inserted. On postoperative MRI, the up migrated disc was removed clearly, and the cervical cord and nerve roots were released well (Figure 2). The operative time was about 185 minutes. Blood loss was 110 cc. The patient reported improved posterior neck pain and right radiating pain with a reduction in NRS from 8 to 3, and improved posterior neck movement compared to the preoperative state.
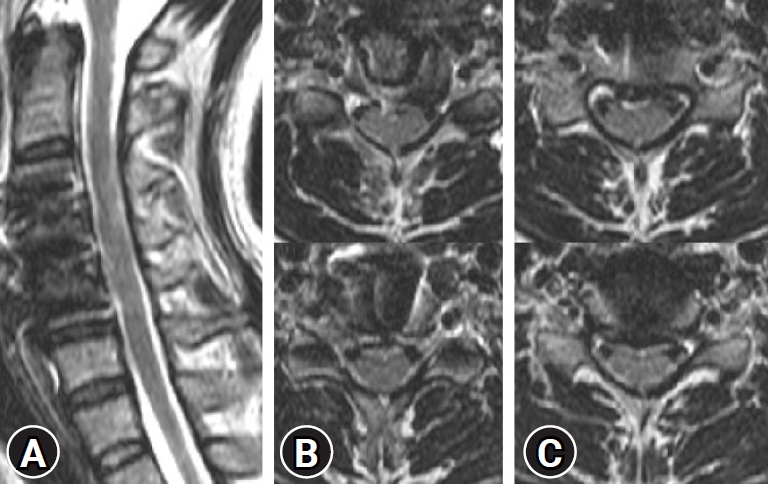
Postoperative images of the up migrated cervical disc herniation at C3-4, C4-5 level on MRI. (A) A mid-sagittal image on T2 weighted MRI. (B) Axial images at C3-4 level on T2 weighted MRI. (C) Axial images at C4-5 level on T2 weighted MRI.
2. Case 2
In November 2021, a 56-year-old man presented with a six-week history of left posterior neck pain and bilateral radiating pain. The pain as evaluated by NRS was 8. Weakness of left elbow flexion and extension, as well as left hand grip as assessed by Manual muscle test (MMT), was Grade 3. Preoperative MRI and CT showed non-calcified left central and foraminal disc extrusion with up migration to the upper level on C6-7, and non-calcified right central disc extrusion with segmental type ossified posterior longitudinal ligament (OPLL) on C5-6 (Figure 3). Electromyography (EMG) showed myelopathy on C5-6.
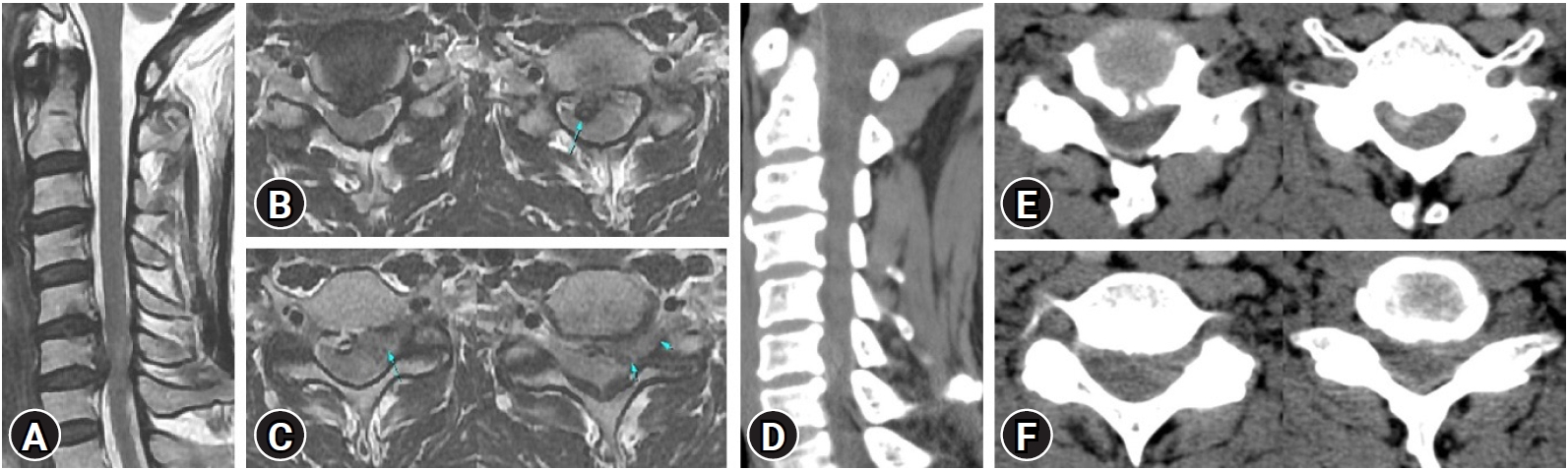
Preoperative images of the up migrated cervical disc herniation at C5-6, C6-7 level on MRI and CT. (A) A mid-sagittal image on T2 weighted MRI. (B) Axial images at C5-6 level on T2 weighted MRI. (C) Axial images at C6-7 level on T2 weighted MRI. (D) Mid-sagittal images on CT. (E) Axial images at C5-6 level on CT. (F) Axial images at C6-7 level on CT.
After informed consent was obtained from the patient, ACDF on the C5-6, C6-7 level was performed. Because of posterior bony spurs, C5-6 level showed dural adhesion, and the disc extrusion was cautiously removed. No injuries to the dura, cord, or nerve root were observed. We inserted 6mm high PEEK cages on C5-6, C6-7 and an anterior plate. Postoperative MRI showed that the cervical cord and nerve roots were decompressed sufficiently (Figure 4). The operative time was approximately 225 minutes. Blood loss was 230 cc. Following the procedure, the patient reported an improvement in left posterior neck pain and bilateral radiating pain (postoperative NRS=2).
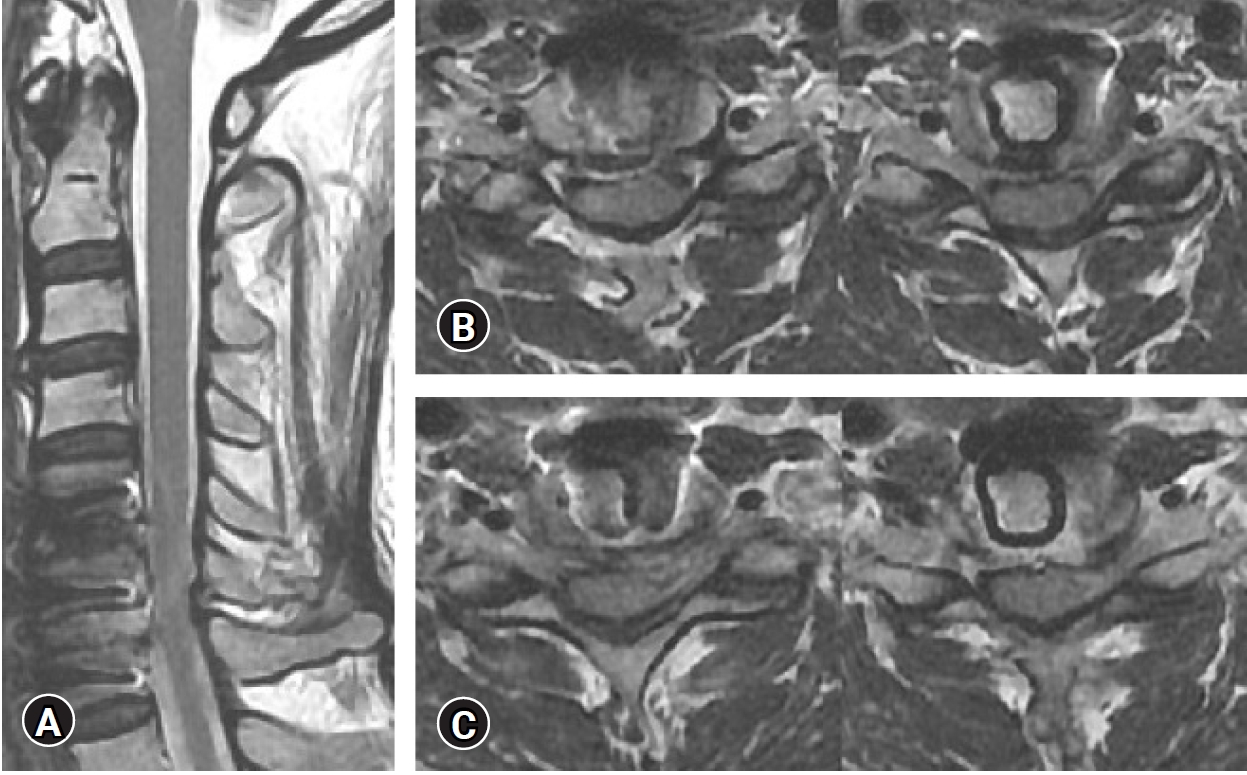
Postoperative images of the up migrated cervical disc herniation at C5-6, C6-7 level on MRI. (A) a mid-sagittal image on T2 weighted MRI. (B) Axial images at C5-6 level on T2 weighted MRI. (C) Axial images at C6-7 level on T2 weighted MRI.
3. Technical notes
Under general anesthesia, the Smith-Robinson approach to the relevant level, discectomy, and endplate preparation are the same as the process of ACDF. The posterior annulus fibrosus and posterior longitudinal ligament (PLL) were removed. The posterior margins of the vertebral body between the center of PLL and foramen were removed within 5 mm using Kerrison punches. With continual disc irrigation, the highly up migrated disc was removed using 5 mm and 10 mm McCulloch angled ball-tipped probe. Bilateral neural foramens were decompressed sufficiently using a high speed drill. After surgical decompression, the cervical cord was pulsated, and the exiting nerve roots were freed. No injuries to the dura, spinal cord, and nerve roots were reported. Cages and an anterior plate were inserted on the target level.
DISCUSSION
ACDF is a widely accepted surgical treatment option for degenerative cervical disc diseases. However, if there is significant up migration of the disc, use of the anterior discectomy approach may be limited due to hidden discs being located behind the vertebral bodies. Most authors advocate treatment with corpectomy instead of anterior discectomy for up migrated cervical disc to the upper level, which allows for the hidden fragments to be fully exposed and clearly removed [3].
ACCF is associated with a relative high rate of implant-related failure. Although these failures could be lessened by implementing additional posterior fixation, the supplemental surgery can increase morbidity, hospital stay and costs [5,6]. Indeed, a recent large-scale cohort study concluded that patients treated with ACCF were more likely to require surgical revision compared to patients treated with ACDF [7]. For elderly patients and those with comorbidities, ACCF is associated with a higher rate of complications, thus more extensive perioperative evaluation and planning are necessary [8]. Due to the drawbacks of ACCF, ACDF can be considered for mild to moderate migrated disc herniation [3].
The major concerns for anterior discectomy are missing migrated fragments behind the vertebral body and more traumatic to the cervical cord than ACCF [1,2]. Several studies reported the “transcorporeal” or “transvertebral” approach, which enable treatment for cervical disc herniation without fusion [9-11]. To remove highly up migrated cervical disc completely, the transcorporeal herniotomy was combined with ACDF. Choi et al. [12] reported a favorable outcome without missing fragments and cord injury. However, this combined approach was applied to the only one level.
To prevent these two problems, some technical notes were combined with ACDF in our study: 1. The posterior margins of the vertebral body between the center of PLL and foramen are removed within 5 mm using Kerrison punches. 5 mm McCulloch angled ball-tipped probe is used to measure 5 mm. Extruded disc fragments are migrated upward beside the center of PLL, because the center of PLL is tightly attached to the vertebral body. 2. The hidden space should be explored carefully to remove highly sequestrated disc using 5 mm and 10 mm McCulloch angled ball-tipped probe. McCulloch angled ball-tipped probe is round, the ball-tipped probe is safer than other probes (Figure 5). The exploration must be done not only upward and downward but also laterally. 3. During the exploration disc saline irrigation should be performed continually to avoid trauma to the cord and remove the remnant fragment efficiently. 4. Sufficient decompression of the cord can be confirmed by the pulsation of the cord. Raynor [13] reported utilizing intraoperative ultrasonography to immediately assess the decompression of cervical cord during ACDF. That might be also used to verify enough decompression. We documented that favorable outcomes without these problems, and Wang et al. [3] supported these lumbar probing techniques with successful results of removing highly up migrated cervical disc herniation.
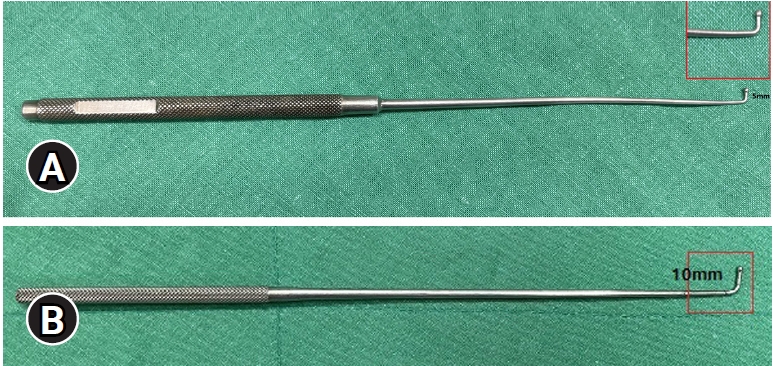
Images of McCulloch angled ball-tipped probes. (A) Images of 5 mm McCulloch angled ball-tipped probe. (B) An image of 10 mm McCulloch angled ball-tipped probe.
In the cases of one or two level highly up migrated cervical disc herniation to the upper level, this lumbar probing technique without partial corpectomy can be applied the first. If severe dural adhesion, including OPLL, is encountered, combined anterior approach with transcorporeal herniotomy will be recommended. In the cases of up migrated cervical disc herniation, the transcorporeal approach without fusion will be considered.
ACDF is utilized in these two methods. They have merits and demerits of ACDF. In the lumbar probing technique, there are difficulties in confirmation of remnant disc fragments and epidural bleeding control. In the combined approach, the vertebral passage facilitates check for the remnant fragments and control of epidural bleeding [12]. Size, location, and trajectory of the passage will be considered carefully due to the risk of vertebral fracture and complete removal of the migrated disc [14].
CONCLUSION
In conclusion, ACDF can be feasible in patients with symptomatic up migrated cervical disc herniation to the upper level behind the vertebral body, providing favorable treatment outcomes without perioperative complications.
Notes
No potential conflict of interest relevant to this article.