Postoperative Horner Syndrome: A Case Report Describing a Rare Complication After Anterior Cervical Discectomy and Fusion
Article information

Abstract
The gold standard for correcting cervical degenerative disc disease (CDDD) is anterior cervical discectomy and fusion (ACDF), which is a safe, effective procedure. Horner syndrome (HS) is an extremely rare complication immediately post-ACDF due to impairment of the sympathetic trunk. Herein, we present the case of a 48-year-old woman with CDDD-related pain and radiculopathy who was counselled and consented for C5–6 and C6–7 ACDF. ACDF was performed with standard anterior left-sided incisions at appropriate levels. Unlike our usual practice, deeper-toothed retractors were employed for better exposure. Two cages were inserted at C5–6 and C6–7. The procedural time was standard (180 minutes), without intraoperative complications. The patient experienced significant symptom relief immediately post-ACDF, but developed sudden onset left-sided HS, with ptosis, miosis, and anhidrosis, approximately 48 hours post-ACDF. At a 2-week postoperative follow-up, she exhibited clinical improvement, and by 12 weeks, her HS had completely resolved. To our knowledge, this case is the first documented instance of delayed-onset HS post-ACDF. It may be associated with the type of retractors used, resulting in neuropraxia or strain on the sympathetic chain ganglia. We recommend adequate exposure while minimizing excessive retraction of the longus colli muscle to reduce irritation to the sympathetic trunk.
INTRODUCTION
A highly efficacious and safe procedure that is minimally-invasive and has withstood the test of time [1,2], anterior cervical discectomy and fusion (ACDF) has become the mainstay for managing cervical radiculopathy and myelopathy in individuals who have unsuccessfully attempted a trial of conservative management in the setting of symptomatic degenerative disc disease (DDD) [2,3].
Despite being a relatively safe procedure and increasing numbers done in an ambulatory setting, as with all procedures, there are still bound to be complications that may arise, including dysphagia, oesophageal perforation, C5 nerve palsy, slippage of prostheses, recurrent laryngeal nerve injury, haematoma, vascular injury, infection and Horner syndrome (HS) [4–6]. HS in the setting of ACDF manifests as ipsilateral ptosis, miosis and anhidrosis of the affected side, and arises when the sympathetic trunk, situated just lateral to the medial border of the longus colli muscle (LCM), is damaged at any point in the neck [7], most commonly during lateral dissection of the LCM or placement of retractor blades above or on the LCM [5,7]. The sympathetic trunk is also more likely to be damaged at a lower level as it is located closer to the medial border of the LCM at the C6 level than the C3 level [8,9]. HS is thus an extremely rare complication post-ACDF with an incidence of 0.6%, but likely underreported in mild cases, with a more recent study by Ashour et. al [10] showing that 4.8% of patients developed post-ACDF HS, especially if performed at lower cervical levels [3-6,8,11]. Thus far the literature suggests that post-ACDF HS tends to develop immediately postprocedure with 80% of cases being left-sided HS and the C5–6 being the most frequently level [8,10-12].
While most patients who have post-ACDF HS resolves spontaneously and completely within a few weeks, there have been reports on persistent HS ranging 0.6% to 3.4% [3,5,7,8]. While the exact reason for persistence of HS is unknown, it is postulated that resolution of post-ACDF HS is determined by its cause of damage – retraction injuries resolve spontaneously while complete severing of the sympathetic chain will cause permanent HS [7,13,14].
While HS may not be life-threatening, it is still an important complication to be aware of and counselled for as its effects can be highly distressing to an individual, especially when the effects of HS can range from a few weeks to possible permanence. Furthermore, coupled with the fact that most CDDD requiring ACDF occurs at the lower cervical levels, the risk of causing HS post-ACDF is higher as well. It is thus important to understand the significance of proper surgical technique and possible causes to reduce the risks of HS.
To the best of our knowledge, this case study represents the first documented instance of delayed-onset HS following ACDF. We postulate that it may possibly be associated with the type of toothed retractors used during the surgery, which might have caused neuropraxia or strain on the sympathetic chain ganglia.
CASE REPORT
The patient is a 48-year-old Chinese lady with a past medical history of hyperlipidaemia and asthma. She presented to clinic with acute on chronic neck pain with left C6 and C7 radicular pain and numbness. Visual analogue scale (VAS) scores were 10/10 in the neck and left upper limb preoperatively, and 6/10 in the left upper limb for radicular pain. Physical examination revealed no motor, sensory or coordination deficits in both upper and lower limbs bilaterally with no functional impairment (Table 1). Written informed consent for publication was obtained from the patient.
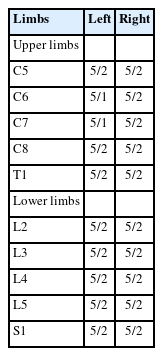
Preoperative ASIA scores of both upper and lower limbs
Radiological investigation showed degenerative changes from anterior osteophytes and uncovertebral joint hypertrophy. T2-weighted magnetic resonance imaging of the cervical spine in axial and sagittal cuts (Figure 1) revealed degenerative changes in the cervical spine with severe bilateral foraminal narrowing at the level of C5–6 and C6–7 with compression of exiting C6 and C7 nerve roots at respective levels.
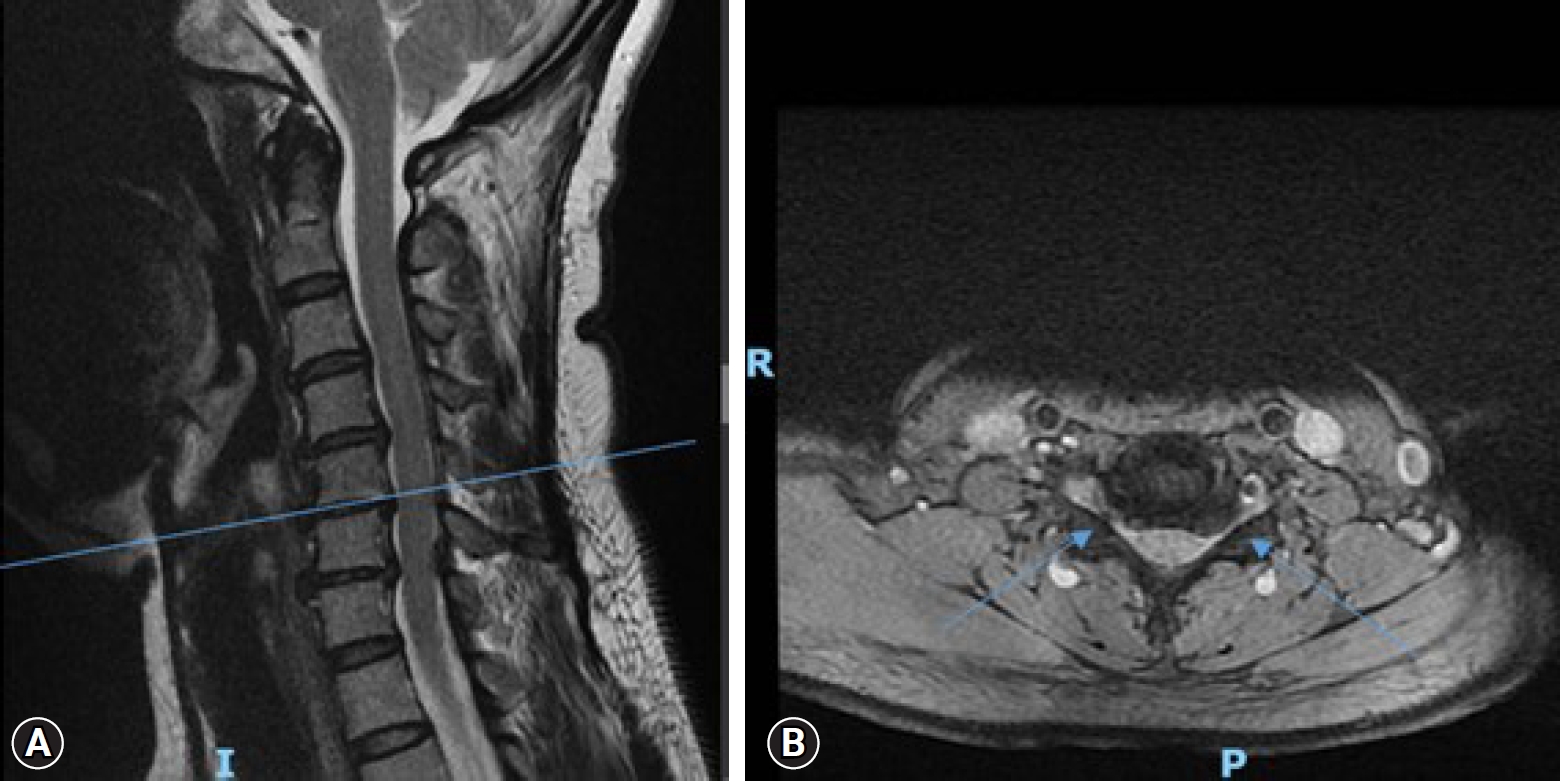
C5–6 level. Arrows pointing towards disc-osteophyte complex indents the spinal cord causing moderate spinal canal stenosis. No cord signal change. Ligamentum flavum thickening and uncovertebral hypertrophy produce bilateral foraminal stenosis with compression of exiting C6 nerve roots. (A) Sagittal cut of T2-weighted magnetic resonance imaging (MRI). (B) Axial cut of T2-weighted MRI at C5-6 level.
The patient was counselled for and consented to undergo ACDF of the C5–6 and C6–7 levels under general anaesthesia. A standard anterior approach with left-sided incision was made at the respective levels under intraoperative imaging (Figure 2A) and placement of Kasper pins (Figure 2B). A cut was made on the left from the midline at the C5–6 level obliquely to the posterior border of the sternocleidomastoid. The investing fascia was incised and the platysma split with finger. The anterior border of the sternocleidomastoid was identified and fascia incised before retracting laterally. Strap muscles and the carotid sheath were retracted medially and laterally respectively. Pretracheal fascia was then incised. The LCMs and anterior longitudinal ligament were split and retracted laterally, taking care to avoid the sympathetic chain, and subperiosteal dissection done to reveal the anterior surface of the vertebral body. Contrasting with our usual practice, deeper-toothed tubular retractors (Figure 3) were employed for better exposure. Anterior decompression of the nerve was then performed under microscopic guidance. The impacted discs at C5–6 and C6–7 were removed and loaded with allogenic bone graft and subsequently compacted. After decompression, the ball tip probes could easily pass through the foramina at both levels bilaterally. Implants used were Zimvie ROI C (Zimmer Biomet, Warsaw, IN, USA) with 5.0-mm × 12-mm × 14-mm anatomical cervical cage secured with 2 H5 5.5-mm plates each at C5–6 and C6–7. Incisions were closed in layers with Vicryl 2/0 interrupted to the platysma and Vicryl 3/0 interrupted buried dermal-subdermal sutures, followed by Stratafix Spiral Monocryl Plus as a continuous subcuticular running suture. Standard procedural time was taken for 2 levels at 180 minutes.
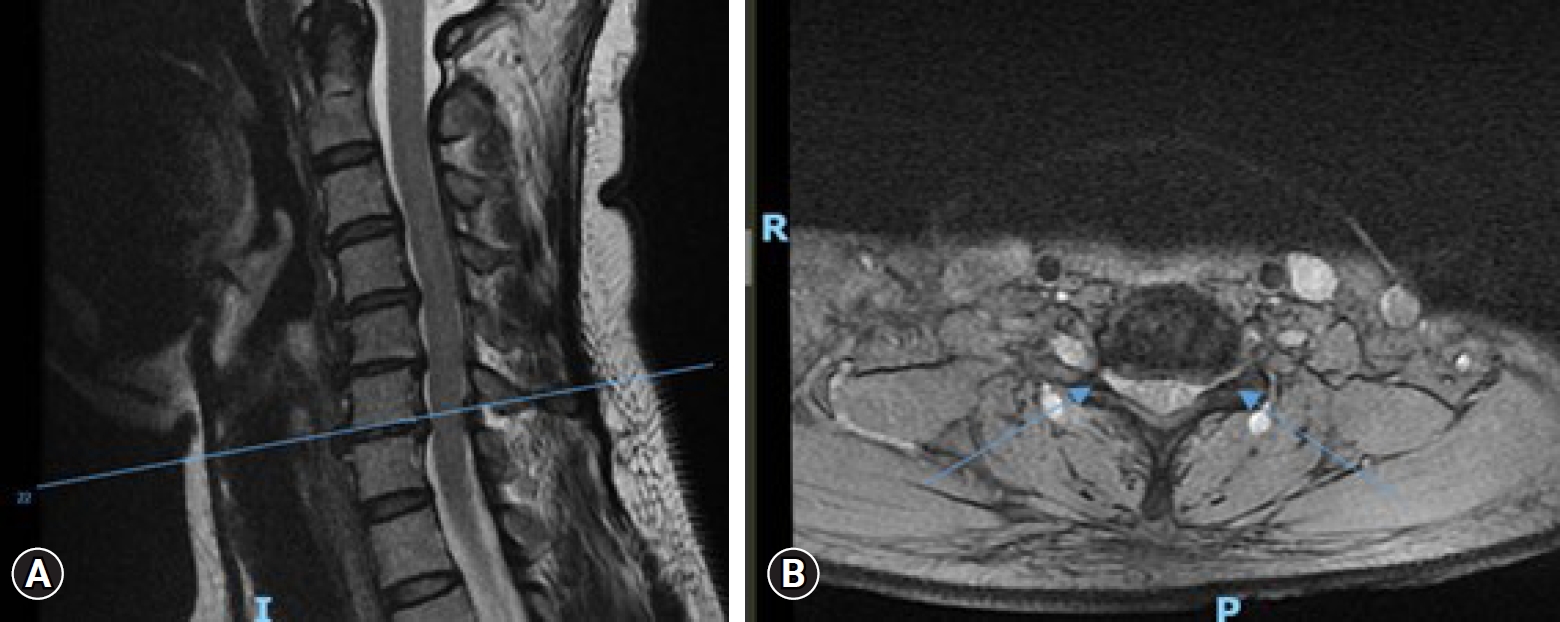
C6–7 level. Arrows pointing towards the disc-osteophyte complex and ligamentum flavum thickening causing moderate spinal canal stenosis. No cord signal change. Uncovertebral hypertrophy with bilateral severe foraminal stenosis with compression of bilateral C7 nerve roots. (A) Sagittal cut of T2-weighted magnetic resonance imaging (MRI). (B) Axial cut of T2-weighted MRI at C6-7 level.

Intraoperative imaging machine used intraoperatively.
Postoperative protocol: IV cefazolin was given for 24-hour postsurgery. The patient was cleared in ambulation for home by the physiotherapist and given a soft brace for 2 weeks. Subsequently, she had monthly physiotherapy sessions for muscle stretching and strengthening exercises of the neck and upper limb. She was discharged with oral analgesia and pregabalin 75 mg twice a day for a month. Her wound was exposed 14 days postoperatively.
The patient was well on postoperative day 1, VAS scores 0/10 with resolution of radiculopathic symptoms and no sensory or motor deficits, but subsequently developed left-sided Horner’s 48-hour post-ACDF, presenting with left-sided ptosis, miosis and anhidrosis. The patient was then initiated on a course of oral prednisolone 20 mg once in the morning for 5 days.
The patient was followed up prospectively at post-op at 2, 6, 12, 16 and 24 weeks and showed improving ptosis and symptoms of HS (Figures 4–10). Marginal reflex distance 1, which is the distance between the upper eyelid margin to the reflection of point source of light (in the middle of the pupil) (Figure 11), was used as an objective method [15] to assess the improvement in the patient’s ptosis (Table 2). VAS scores remained at 0/10 at each follow-up.

Arrows pointing to Kaspar pins used to identify the correct cervical vertebral body with the help of intraoperative imaging.
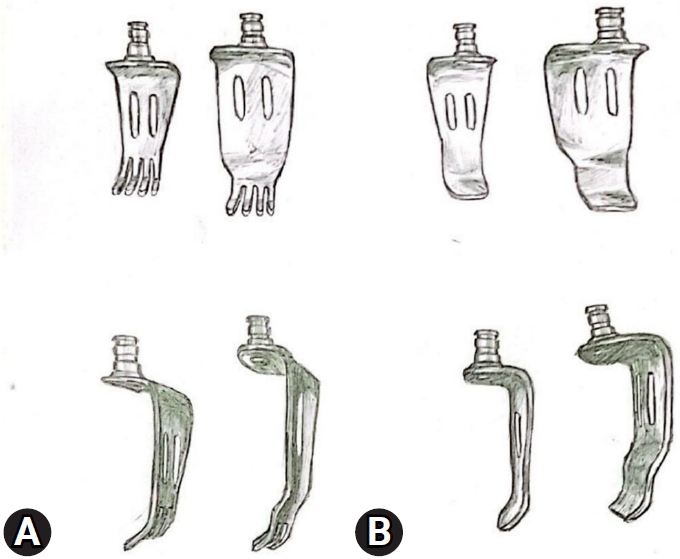
(A) Toothed retractors used in this operation (front and side views from top to bottom respectively) as compared to (B) nontoothed retractors used in usual practice.

Clinical photograph showing left-sided ptosis on postoperative day 2.

Clinical photograph showing progress of left-sided ptosis at 2-week follow-up.

Clinical photograph showing progress of left-sided ptosis at 6-week follow-up.

Clinical photograph showing progress of left-sided ptosis at 12-week follow-up.

Clinical photograph showing progress of left-sided ptosis at 16-week follow-up.
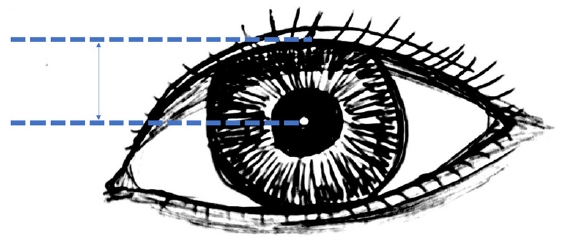
Figure shows the marginal reflex distance 1.
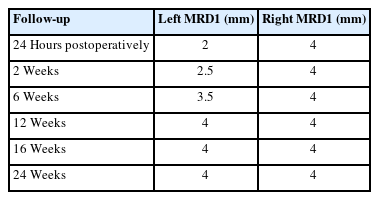
MRD1 scores at various follow-up durations
DISCUSSION
Post-ACDF HS is a recognized but rare postoperative complication, with various factors showing possible links to a higher incidence, such as the duration of surgery [10], type of anaesthesia [16], and the number and level of fusions [8,10,11,17]. Notably, there have been no reported cases of delayed-onset HS following ACDF beyond 48-hour postsurgery.
It has been cited in the literature that the excessive retraction of the LCM, [8,10,11,17] is associated with a higher risk of HS. However, an apparent gap exists in the literature regarding the influence of retractor type and risk of HS, likely because of the rarity of HS. In our institution, the conventional practice involves the use of blunt, nontoothed tubular retractors. However, in this case, we deviated from our norm by employing blunt toothed retractors in an attempt to achieve improved exposure. While challenging to substantiate, we hypothesize that the use of toothed retractors might concentrate pressure on specific points, potentially causing accelerated microdamage to the sympathetic chain. This damage could accumulate during the surgical procedure, leading to minor neuropraxia of the sympathetic chain. The gradual accrual of damage might surpass the body's clearance mechanisms, resulting in nerve damage and, consequently, the delayed onset of HS. We do acknowledge that other factors in this case may have confounded and increased the chance of HS, including the 180-minute surgery duration [10], a left-sided incision and approach to the anterior cervical spine [11], and the cervical level being done at C5–6 [8,10,11,17,18], all known to elevate the incidence of HS.
In this instance of delayed-onset post-ACDF HS, the recovery period appeared prolonged compared to immediate postoperative HS. Conventional post-ACDF HS cases, according to a meta-analysis, typically show the majority of patients resolving completely within 6 weeks, with an average time for initial improvement being 4.3 weeks [10]. Fortunately, we observed complete resolution of HS in our case, but it took 12 weeks, nearly double the typical recovery period for post-ACDF HS. It remains challenging to ascertain whether this prolonged recovery is specific to delayed-onset HS as a more chronic pathology or if other contributing factors are at play. Further studies may be warranted to investigate the matter.
Several case studies [19,20] have reported marked clinical improvement in HS postthyroidectomy after a course of oral steroids, which points towards the possible role of postoperative steroids in the resolution of HS. However, the role of corticosteroids in the management of post-ACDF HS remains unclear, as no studies have explored the relationship between corticosteroid use and the duration of HS post-ACDF.
Given that the likely pathology of this HS was traumatic and inflammatory, a trial of steroids was administered. It is true that, conversely, steroids could have impaired the healing and natural neurological recovery, thus potentially slowing down complete resolution. However, it is challenging to ascertain, and further assessments and studies would be warranted to discover any implications regarding the speed of recovery of post-ACDF HS and corticosteroid use.
This case report is limited by its small number and rarity of the presentation, and hence further research on the possible causes of delayed presentation of HS and its risk factors could be done to lower the risk of such complications postoperatively.
CONCLUSION
HS post-ACDF is rare, and this case study presents the first documented occurrence of delayed-onset HS following ACDF. We postulate that it may be possibly linked to the use of toothed retractors, causing accelerated microtrauma to the sympathetic chain ganglia. Proficient knowledge of the anatomy of the cervical sympathetic trunk underscores the ability to prevent iatrogenic HS. Care should also be taken intraoperatively to avoid excessive traction of the LCM to prevent unnecessary injury to the sympathetic trunk. We suggest for further studies to determine the cause, pathophysiology, and optimal management for such cases.
Notes
Conflict of Interest
The authors have nothing to disclose.
Funding/Support
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.